
Understanding Two-Phase Orthodontic Treatment: A Comprehensive Guide to Early Intervention for Optimal Dental Development

Two-phase orthodontic treatment represents a strategic and timely approach to guiding a child’s dental and jaw development, diverging from the traditional method of waiting until all permanent teeth have erupted. This treatment plan unfolds in two distinct stages, meticulously timed to coincide with crucial periods of a child’s growth and dental maturation. The American Association of Orthodontists (AAO) advocates for early orthodontic evaluation, recommending a child’s first check-up no later than age seven. This proactive stance aims to leverage periods of active growth to guide jaw development, optimize the alignment of teeth, and establish the most favorable conditions for the eruption of permanent teeth, thereby mitigating the severity of potential future problems.
This targeted intervention is typically employed when an orthodontist identifies specific early changes that can significantly enhance a child’s long-term oral health and functional capabilities. By addressing issues such as jaw discrepancies, severe crowding, or specific bite problems during formative years, two-phase treatment can reduce the complexity and duration of later corrective measures, or even prevent the need for more invasive procedures down the line. While a single phase of comprehensive orthodontic treatment remains the appropriate path for many children, a qualified orthodontist plays a crucial role in assessing individual needs and determining the most suitable treatment plan. This guide, drawing upon insights from the AAO, delves into the specifics of two-phase orthodontic treatment, exploring its definition, the conditions it addresses, and the criteria for identifying ideal candidates.
Defining the Two-Phase Approach to Orthodontic Care
At its core, two-phase orthodontic treatment is structured into two sequential stages: Phase One, also known as early or interceptive treatment, and Phase Two, which constitutes comprehensive orthodontic treatment. Phase One typically commences when a child presents with a mixed dentition, meaning a combination of primary (baby) and permanent teeth. This initial phase capitalizes on the child’s active growth to make fundamental corrections. Phase Two then follows, generally initiating when most, if not all, permanent teeth have emerged, focusing on the precise alignment and final positioning of the dentition.
Phase One treatment primarily involves interventions designed to promote proper jaw growth and development, with the overarching goal of minimizing the extent and complexity of future orthodontic needs. Common appliances utilized during this phase include palate expanders, which widen the upper jaw to create space and correct crossbites; tongue cribs or lingual arches, used to break habits like thumb-sucking or tongue thrusting and maintain space; and in some instances, limited braces applied to a select few permanent teeth. The analogy of scaffolding around a building under construction effectively illustrates Phase One. Just as scaffolding guides and supports the initial structural development of a building, Phase One guides a child’s growing jaws, reducing the severity of malocclusions (bad bites). This foundational work then allows Phase Two to build upon the established improvements, enabling a more straightforward and predictable process for the final correction and fine-tuning of the child’s bite.
The Rationale Behind Early Orthodontic Intervention: A Shift in Philosophy
The philosophy underpinning two-phase orthodontics represents a significant evolution in dental care, moving from a purely corrective model to one that emphasizes prevention and early guidance. Historically, orthodontic treatment was largely initiated during adolescence, once all permanent teeth had erupted. However, decades of clinical research and observation, largely spearheaded by organizations like the AAO, have highlighted the profound advantages of intervening during a child’s active growth phases.
The human jaw and facial bones undergo significant development during childhood, offering a window of opportunity to influence growth patterns in ways that are simply not possible once growth has ceased. Addressing issues like a constricted upper jaw, an underdeveloped lower jaw, or severe space deficiencies early can prevent these problems from becoming more entrenched and difficult to resolve later. For instance, correcting a crossbite in a young child can prevent asymmetrical jaw growth and potential temporomandibular joint (TMJ) issues. Similarly, creating adequate space for erupting permanent teeth can reduce the need for future tooth extractions. This proactive approach not only aims for better clinical outcomes but also seeks to reduce the overall treatment burden on the patient in the long run.
Who Benefits Most: Identifying the Ideal Candidate for Two-Phase Treatment
While designed for children, two-phase orthodontic treatment is not a universal requirement. Many common orthodontic issues can be effectively resolved with a single phase of comprehensive treatment during adolescence. An orthodontist will recommend a two-phase approach only after a thorough evaluation reveals that early intervention is critical to supporting a healthy, functional bite and overall facial development as the child matures.
Two-phase treatment is typically considered when early growth guidance can effectively address specific concerns such as significant jaw development discrepancies (e.g., severe underbites or overbites), severe crowding, problematic bite relationships (like anterior or posterior crossbites), or issues with the eruption path of permanent teeth. The primary objective of Phase One is not to achieve "perfection" but rather to "set the stage" for healthier, more harmonious development. The decision to pursue a two-phase approach is made when an orthodontist determines that a child is likely to develop a severe malocclusion or jaw problem, or faces a high risk of damage to permanent teeth, and that Phase One treatment has a substantial likelihood of reducing the severity of these conditions and mitigating associated risks. This targeted approach ensures that resources are allocated where they can yield the most significant developmental benefits.
How Phase One Treatment Works: Guiding Growth and Creating Space
Phase One treatment typically commences when a child still possesses a mix of primary and permanent teeth, often between the ages of 7 and 10. During this critical developmental window, an AAO orthodontist can strategically guide jaw growth, facilitate the creation of adequate space for the eruption of permanent teeth, or correct bite problems that are more amenable to influence while the child’s skeletal structure is still developing.
The specific interventions during Phase One can vary widely based on the diagnosed issue. Treatment may involve the use of braces on a limited number of teeth, or another orthodontic appliance, which can be either fixed (e.g., a palate expander) or removable (e.g., a retainer-like device). The orthodontist selects the most appropriate option based on the child’s unique needs and the specific goals of the treatment plan. In certain scenarios, the strategic removal of one or more baby teeth might be recommended to create necessary space, thereby allowing permanent teeth to erupt into more favorable positions and reducing future crowding.
Common Phase One Methods and Their Applications:
Orthodontists meticulously select corrective devices based on the specific problem being addressed, the child’s current stage of growth, and the overarching treatment plan. Common Phase One approaches and their primary functions include:
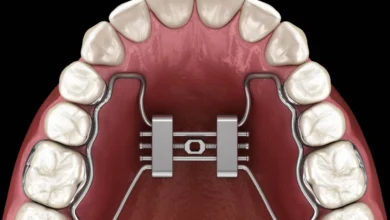
- Palate Expanders: These devices, often fixed to the upper molars, are used to gradually widen a narrow upper jaw. This expansion can correct posterior crossbites, create space for crowded permanent teeth, and improve breathing by widening the nasal passages. Early expansion is highly effective because the upper jaw (maxilla) is still developing and its two halves have not yet fused.
- Space Maintainers (Lingual Arches, Band-and-Loop): If a baby tooth is lost prematurely due to decay or injury, a space maintainer can be used to prevent adjacent teeth from drifting into the vacant space. This ensures that sufficient room is preserved for the eventual eruption of the permanent tooth.
- Tongue Cribs or Habit Appliances: These small, fixed devices are placed behind the upper front teeth to discourage habits such as thumb-sucking or tongue thrusting, which can significantly impact jaw development and tooth alignment. Breaking these habits early can prevent open bites and other malocclusions.
- Partial Braces: In some cases, braces may be applied to a limited number of permanent teeth to correct specific issues like severe crowding of the front teeth, close gaps, or upright teeth that are erupting at an incorrect angle.
- Headgear or Facemasks: For more significant jaw discrepancies, such as an underdeveloped upper jaw or an overdeveloped lower jaw, external appliances like headgear or facemasks may be used to guide jaw growth in the desired direction. These are typically worn for a prescribed number of hours each day.
- Removable Retainers/Appliances: Sometimes, removable appliances are used to achieve minor tooth movements or to hold space.
The efficacy of a Phase One plan hinges on connecting the choice of corrective device directly to the end goal: fostering a healthier bite and establishing an optimal path for the eruption of permanent teeth.
The Interphase: A Crucial Resting Period
A defining characteristic of two-phase treatment is the resting period that occurs between Phase One and Phase Two. It is crucial to understand that these phases are not conducted back-to-back or simultaneously. After the completion of Phase One, most children enter this interphase, allowing for a period of natural growth and the continued eruption of remaining permanent teeth. This break is vital for several reasons: it gives the jaw and teeth time to respond to the changes initiated in Phase One, consolidate improvements, and allows the orthodontist to observe the natural progression of dental development.
During this resting period, the orthodontist remains involved, typically scheduling periodic check-ups to monitor the child’s progress. These appointments allow the orthodontist to evaluate the stability of the changes achieved in Phase One, assess the eruption patterns of permanent teeth, and meticulously plan the timing and specific goals for Phase Two. This ongoing oversight provides significant reassurance to families, ensuring that the child’s orthodontic needs are continuously managed and adapted as growth and tooth eruption unfold.
How Phase Two Treatment Works: Achieving Comprehensive Alignment
Phase Two treatment usually commences when most, if not all, of the child’s permanent teeth have erupted, typically during early to mid-adolescence. While Phase One focused on establishing a healthy developmental environment and correcting foundational jaw issues, Phase Two centers on the precise placement of all permanent teeth into their ideal positions. The objectives of Phase Two are to achieve strong functional occlusion (how the teeth fit together), ensure a healthy bite, and create an aesthetically pleasing smile.
Phase Two often aligns with what many people traditionally envision as orthodontic treatment, primarily utilizing full braces or clear aligners. Braces, comprising brackets bonded to each tooth and connected by an archwire, exert continuous, gentle forces to guide teeth into their correct positions. Modern braces offer various options, including traditional metal, ceramic (tooth-colored), and lingual (behind the teeth) braces. Clear aligners, such as Invisalign, offer a more discreet alternative, using a series of custom-made, removable plastic trays to gradually shift teeth. The choice between braces and aligners depends on the complexity of the case, patient preference, and compliance. During Phase Two, the orthodontist refines the alignment of teeth and perfects the interdigitation of the upper and lower jaws to ensure a stable and functional bite.
Are Baby Teeth Moved for Cosmetic Reasons in Phase One?
A common concern among parents considering Phase One treatment is whether the movement of baby teeth is driven by cosmetic considerations. The unequivocal answer is no. The primary focus of Phase One is entirely functional and developmental, not aesthetic. Phase One treatment is specifically reserved for problems that can be most effectively and beneficially addressed during periods of active growth. If baby teeth are shifted or even extracted during Phase One, it is always part of a larger strategy to create necessary space for permanent teeth, guide their eruption path, and influence overall jaw development. Such interventions are critical for establishing a healthier foundation and preventing more severe issues from developing later.
Broader Impact and Implications of Two-Phase Orthodontics
The benefits of two-phase orthodontic treatment extend far beyond merely straightening teeth, encompassing significant health, functional, and psychological advantages for the child.
Health Benefits:
- Reduced Risk of Trauma: Severely protruded upper front teeth are highly susceptible to injury (fractures, avulsions). Phase One can retract these teeth, significantly reducing the risk of accidental trauma, which is a common concern for active children.
- Improved Oral Hygiene: Properly aligned teeth are easier to clean, reducing the risk of plaque accumulation, cavities, and gum disease (gingivitis and periodontitis).
- Enhanced Chewing and Digestion: A well-aligned bite improves the efficiency of chewing, contributing to better digestion and nutrient absorption.
- Reduced Risk of TMJ Issues: Correcting significant bite discrepancies and jaw misalignments early can alleviate undue stress on the temporomandibular joints, potentially reducing the risk of developing painful TMJ disorders in adulthood.
- Better Airway Function: Palatal expansion, a common Phase One procedure, can widen the nasal passages, potentially improving breathing, especially in children with narrow arches and associated airway issues.
Functional Benefits:
- Improved Speech: Certain malocclusions can impede proper tongue placement and articulation, leading to speech impediments. Early correction can facilitate clearer speech development.
- Easier Eating: A functional bite allows for comfortable and efficient biting and chewing of a wider variety of foods.
Psychological Benefits:
- Enhanced Self-Esteem and Confidence: Dental irregularities can be a source of self-consciousness, bullying, and reduced self-esteem in children. Addressing these issues early can significantly boost a child’s confidence and social interactions. A 2017 study published in the American Journal of Orthodontics and Dentofacial Orthopedics highlighted the positive impact of orthodontic treatment on quality of life, including social well-being and emotional health.
Efficiency and Economic Considerations:
- Potentially Simpler Phase Two: By addressing major skeletal and space issues in Phase One, the subsequent Phase Two treatment can often be shorter, less complex, and may even avoid the need for tooth extractions or orthognathic surgery (jaw surgery) that might otherwise be necessary.
- Long-Term Stability: Early intervention can create a more stable foundation for the final bite, potentially leading to more enduring results and reducing the likelihood of relapse.
- Cost-Effectiveness (Long-Term): While two-phase treatment involves an initial investment, it can be more cost-effective in the long run by preventing more severe and expensive problems (e.g., extensive restorative work, surgery) from developing.
Guidance for Parents: Making Informed Decisions
When considering two-phase orthodontic treatment, parents should view it as a meticulously coordinated plan, not two disconnected treatment experiences. It is essential to engage in thorough discussions with the child’s orthodontist. Key questions to ask include: How does Phase One specifically support the objectives of Phase Two? What are the precise changes being targeted in the current phase, and what are the expectations for addressing issues later? Robust answers will clearly link the timing and chosen treatment options to the child’s growth patterns, long-term bite health, and the stability of the final outcome.
It is also beneficial to clarify what constitutes "success" after Phase One. Success might mean successfully creating necessary space, significantly improving a problematic bite relationship, or substantially reducing the severity of an issue, thereby ensuring that Phase Two can be simpler, more predictable, and potentially shorter.
The AAO Recommendation: The Importance of a Timely Evaluation
The American Association of Orthodontists unequivocally recommends that children undergo their first orthodontic check-up no later than age seven. This age is considered optimal because by this point, a sufficient number of permanent teeth have typically erupted (including the first permanent molars and incisors) to allow an orthodontist to accurately identify developing issues with jaw growth and bite alignment. Even if a child’s teeth appear straight to the untrained eye, an orthodontist possesses the specialized knowledge to detect subtle problems that could worsen over time.
Crucially, parents do not need a referral from a general dentist to schedule an orthodontic consultation for their child. Directly booking an appointment with a qualified orthodontist is entirely sufficient. This early evaluation is not a guarantee of immediate treatment but rather a proactive step to assess development and determine if and when intervention might be beneficial.
Finding the Best Treatment for Your Child with an AAO Orthodontist
Two-phase orthodontic treatment stands as a powerful tool in modern orthodontics, particularly when early intervention can profoundly support healthier growth trajectories and the development of a more functional and aesthetically pleasing bite. However, it is imperative to reiterate that it is not a necessary course of action for every child. The decision to pursue a single-phase or two-phase approach rests on a comprehensive evaluation by a specialist.
An AAO orthodontist possesses the advanced training and expertise in growth and development to accurately assess a child’s unique smile and bite. They can provide a clear explanation of whether one phase or two phases make the most sense for your child, and crucially, recommend the precise timing of any intervention based on scientific principles of development, rather than guesswork. Utilizing the AAO’s "Find an Orthodontist tool" (aaoinfo.org/locator) is an invaluable resource for parents seeking a qualified professional in their vicinity to schedule an evaluation today, ensuring their child receives care grounded in expertise and evidence-based practice.







{kind=link}